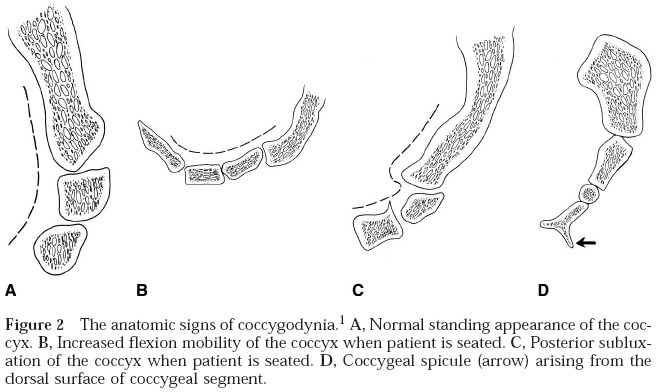
Normal coccyx pivots slightly (5 to 25°) either posterior or anterior with sitting & returns to its original position with standing
Abnormalities of coccygeal segments in seated views have anterior hypermobility >25°
Subluxation or posterior displacement of mobile segment of coccyx is seen when patient is seated
A spicule of distal tip is seen most commonly with an immobile coccyx (<5° of motion with sitting)
Other investigations:
CT of sacrococcygeal region
MRI can show inflammation or subluxxation
Technetium 99m bone scan
Relief with injection of local anaesthetic
Management
Non-operative:
NSAIDs
Analgesics
Rest
Hot baths
Cushion to protect coccygeal region from repetitive trauma
Injection methylprednisolone (40 mg) & bupivacaine (10 mL 0.25%) around side & tip of coccyx (60% cure rate), or into an inflamed sacrococcygeal joint, as shown by MRI
Operative:
Indications
Significant disabling coccydynia with radiographic subluxation
Instability
Coccygeal spicule, particularly on the tip of an immobile coccyx
After non-operative management has failed
Technique
Bowel preparation day prior
Prophylactic antibiotics
Prone position with hips & knees flexed
Vertical incision over coccyx, extending from just above sacro-coccygeal joint into buttock crease without extending into perianal skin, through fascia & gluteus maximus, dissecting directly to bone
All segments removed & end of sacrum smoothed by rasp, rongeur, or burr
Results
90% good to excellent results at 8 years
Complications
Perineal contamination of wound resulting in infection (10%)